
President Donald Trump’s budget includes Medicaid reforms that would restore accountability and improve the federal-state partnership.
Predictably, the left is on the attack, contending that these “cuts” would harm the poor and vulnerable.
In fact, the president’s proposals would reduce improper federal spending, which now exceeds $75 billion annually, preserve public resources for those most in need, and provide states with better incentives to obtain value from the program.
Despite the massive bump up in Medicaid spending from Obamacare’s expansion of it, the president’s budget will not cut Medicaid, but will rather slow the projected increase in spending.
Many of the program’s problems result from the federal government providing an open-ended reimbursement of state Medicaid expenditures.
On average across states, every dollar of Medicaid spending on “traditional” program enrollees, such as the disabled, and low-income children, pregnant women, and seniors, brings in nearly two dollars of federal spending.
For Obamacare’s expansion population of able-bodied, working-age adults, each dollar of state spending brings in nine federal dollars.
Thus, there is a torrent of spending with little accountability and generally poor results. According to economic research, many Medicaid enrollees value benefits from the program at much less than the cost of coverage, suggesting that overall societal welfare can be improved through program redesign.
Unsustainable Spending
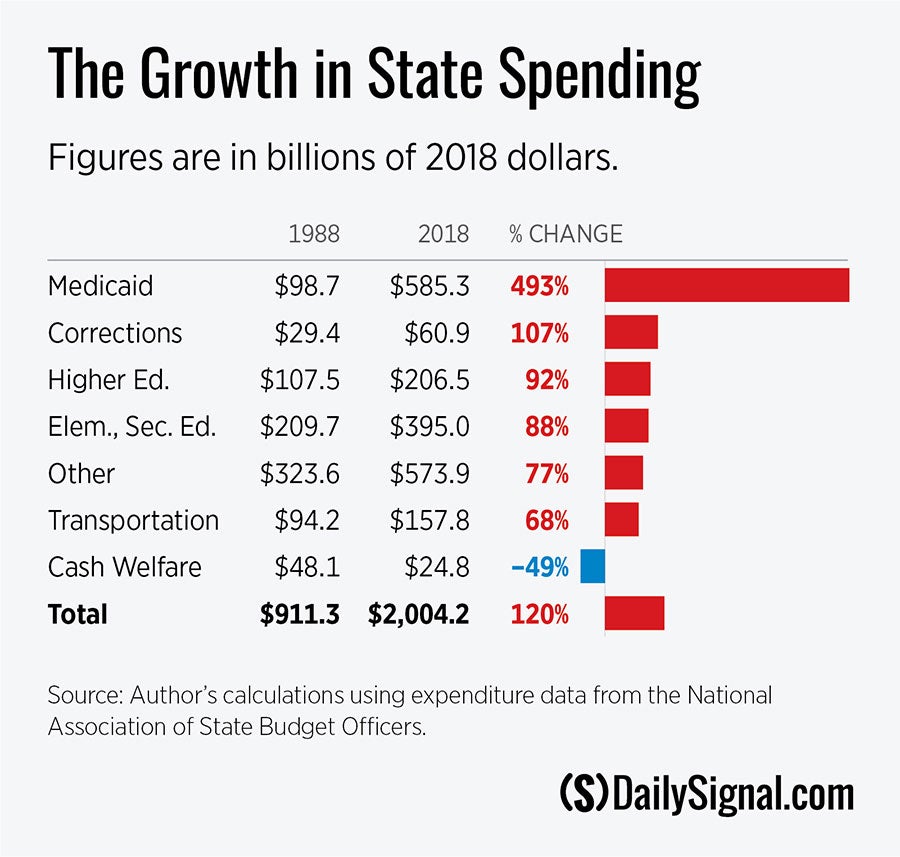
Medicaid spending has exploded over the past three decades—from $98.7 billion in 1988 (in inflation-adjusted 2018 dollars) to $585.3 billion in 2018, a real increase of nearly 500 percent.
One problem is that the open-ended reimbursement of state spending creates an incentive for states to develop essentially fake expenditures in order to maximize federal matching funds.
One such technique involves provider taxes, which Oregon state Rep. Merwyn “Mitch” Greenlick referred to as a “dream tax” for states: “We collect the tax from the hospitals,” the Democrat explained. “We put it up as a match for federal money, and then we give it back to the hospitals.”
Reforming these financing gimmicks has long-standing bipartisan support, with both President Barack Obama’s budgets and the 2010 Simpson-Bowles fiscal commission calling for significant reform.
Crowding Out Other Priorities
Medicaid now represents roughly two-thirds of all federal money received by states. The table below shows the growth in inflation-adjusted state expenditures, by major category, between 1988 and 2018. Medicaid spending grew by nearly 5-1/2 times more than education spending.
Ineligible Enrollees, Massive Improper Spending
When Obamacare’s Medicaid expansion started in 2014, the Centers for Medicare and Medicaid Services stopped doing audits of state Medicaid eligibility determinations.
After a four-year hiatus, those audits resumed in 2018. The audits, along with several others, show that a large percentage of Medicaid enrollees have been improperly enrolled.
One such audit found eligibility problems with more than half of sampled enrollees in California’s Medicaid program.
Largely as a result of eligibility problems, Medicaid’s improper payments now almost certainly exceed $75 billion, or more than 20% of all federal Medicaid expenditures. Before Obamacare, the Medicaid improper-payment rate was 6%.
Discrimination Against the Most Deserving
By providing a higher reimbursement for Obamacare-expansion enrollees, the federal government is now discriminating against the traditional Medicaid populations in favor of the able-bodied, working-age adult population.
That’s unfair to those who Medicaid was intended to serve and leads to some diversion of services away from traditional Medicaid enrollees.
Enormous Medicaid Crowd-Out of Private Coverage
Since Medicaid is heavily subsidized, eligibility expansions encourage individuals to replace private coverage, passing costs to taxpayers.
Economists Jonathan Gruber and Kosali Simon estimated crowd-out at 60 percent for expansions between 1996 and 2002. That means that for every 10 people gaining Medicaid coverage, six of them simply replaced private coverage.
Medicaid also substantially crowds out the market for private long-term care insurance. Crowd-out may be harmful for overall health since private coverage generally provides better access to care than government programs, which pay providers lower rates.
Low value received by many Medicaid enrollees
Numerous studies suggest that the way to best use public resources to improve health is through targeted initiatives focused on individuals who are most likely to benefit from care and through investments in child health.
In contrast, Obamacare’s massive Medicaid expansion produces the most benefit to insurance companies who end up with a sizable profit (as the White House’s Council of Economic Advisers found), as well as hospitals and providers who gain additional payments for services they previously provided for free or at low cost (as prominent economists have found).
In 2008, Oregon utilized a lottery to expand Medicaid to some able-bodied uninsured adults with incomes below 100 percent of the federal poverty level—allowing researchers an important experimental study to assess the impact of gaining Medicaid.
The main takeaway from the study is that the new Medicaid recipients increased the amount of health care they received, including emergency services, but did not show improvement on the three physical-health measures assessed—blood pressure, cholesterol, and blood sugar.
Moreover, as a testament to the low perceived value of the program, 40 percent of people who won the lottery did not end up enrolling in Medicaid.
A study by economists Amy Finkelstein, Nathaniel Hendren, and Ezro Luttmer found that Oregon’s expansion enrollees placed relatively low value on the program, estimating that expansion recipients would have only paid 20 to 40 cents for each dollar that the program spent on their behalf.
The authors found that most of the benefit of expansion accrued to providers who were able to reduce the amount of uncompensated care they provided.
Reforming Medicaid
The federal-state Medicaid partnership needs to be corrected so that the incentives are aligned to focus on maximizing value for program enrollees and not the profits of the health care industry.
Unfortunately, states often concentrate on maximizing federal receipts for Medicaid, rather than being wise stewards of taxpayer dollars and best serving eligible populations.
While the president’s opponents tend to ignore problems with government programs, the administration is attempting to focus resources in ways that most improve enrollees’ health and financial well-being, while at the same time ensuring that taxpayer dollars are not wasted.